DMSO Heals the Gut and Cures Gastrointestinal Diseases
LewRockwell.com
Many common and debilitating GI conditions have rapid and dramatic responses to DMSO.
MidwesternDoctor | midwesterndoctor.com
• Inflammatory bowel diseases, due to a reluctance to examine their root causes, remain an area that medicine struggles with. As such many who suffer from them are subjected to a life of costly healthcare expenses and debilitating complications.
• DMSO is an “umbrella remedy” capable of treating a wide range of challenging ailments due to its combination of therapeutic properties (e.g., reducing inflammation, improving circulation, and reviving dying cells).
• Many of these properties (e.g., healing inflammation, improving circulation, restoring damaged organs, and normalizing parasympathetic function) are uniquely suited to address the underlying causes of gastrointestinal disorders (e.g., DMSO can help regenerate insulin-producing cells in the pancreas).
• A large volume of published data and many user reports show that DMSO often produces remarkable results for a wide range of inflammatory bowel disorders (e.g., Crohn’s disease, ulcerative colitis, IBS, diverticulitis, leaky gut syndrome, or SIBO).
• Likewise, extensive data supports using DMSO to treat injuries to the rest of the GI tract (e.g., gastritis, peptic ulcers, liver cirrhosis, cholecystitis, pancreatitis, peritonitis, amyloidosis) and frequent but frustrating problems such as hemorrhoids, prostate enlargement, and prostatitis.
• This article will review the data demonstrating DMSO’s efficacy for gastrointestinal diseases, along with an examination of the most common protocols used for them and other natural approaches that also aid in the treatment of these common disorders. It will also provide guidelines for general DMSO procurement and use.
Living with an inflammatory bowel disorder (IBD) like Crohn’s disease or ulcerative colitis is a daily balancing act marked by unpredictability. Symptoms such as abdominal pain, urgent diarrhea, and fatigue can flare up without warning, disrupting plans and demanding constant awareness of diet, stress, and bathroom access.
Severe flares can escalate to the point of requiring hospitalization, where intense pain, dehydration, or complications like obstructions necessitate urgent medical intervention, often involving IV treatments or surgery.
During flares, the physical toll—cramping, bloating, and sometimes blood in the stool—can be exhausting, while remission periods offer relief but never erase the underlying uncertainty of potential hospital stays. Beyond the body, IBD carries an emotional weight: frustration from cancelled outings, anxiety about explaining the condition, and the quiet resilience needed to manage (frequently toxic) medications, doctor visits, hospital recoveries, and lifestyle adjustments. Likewise, owing to their complexity and frequent severity, inflammatory bowel diseases are often quite challenging for physicians to manage, hence frequently requiring specialized care.
Note: one highly under appreciated consequence of inflammatory bowel disorders is that they reduce the absorption of key nutrients (e.g., by up-regulating the liver’s production of hepcidin or reducing the ability of the intestinal lining to transport nutrients into the bloodstream) and as such, effectively managing these conditions frequently requires an extensive micronutrient workup.
Recently, I discussed the silent epidemic of chronic constipation (affecting 15-16% of adults), and the remarkable fact that almost all of it (14% of adults) is constipation that has no known cause—resulting in millions being placed on a lifetime of laxatives rather than the actual causes of their constipation being diagnosed and addressed.
Note: after publication, that article was significantly revised with additional treatments for constipation.
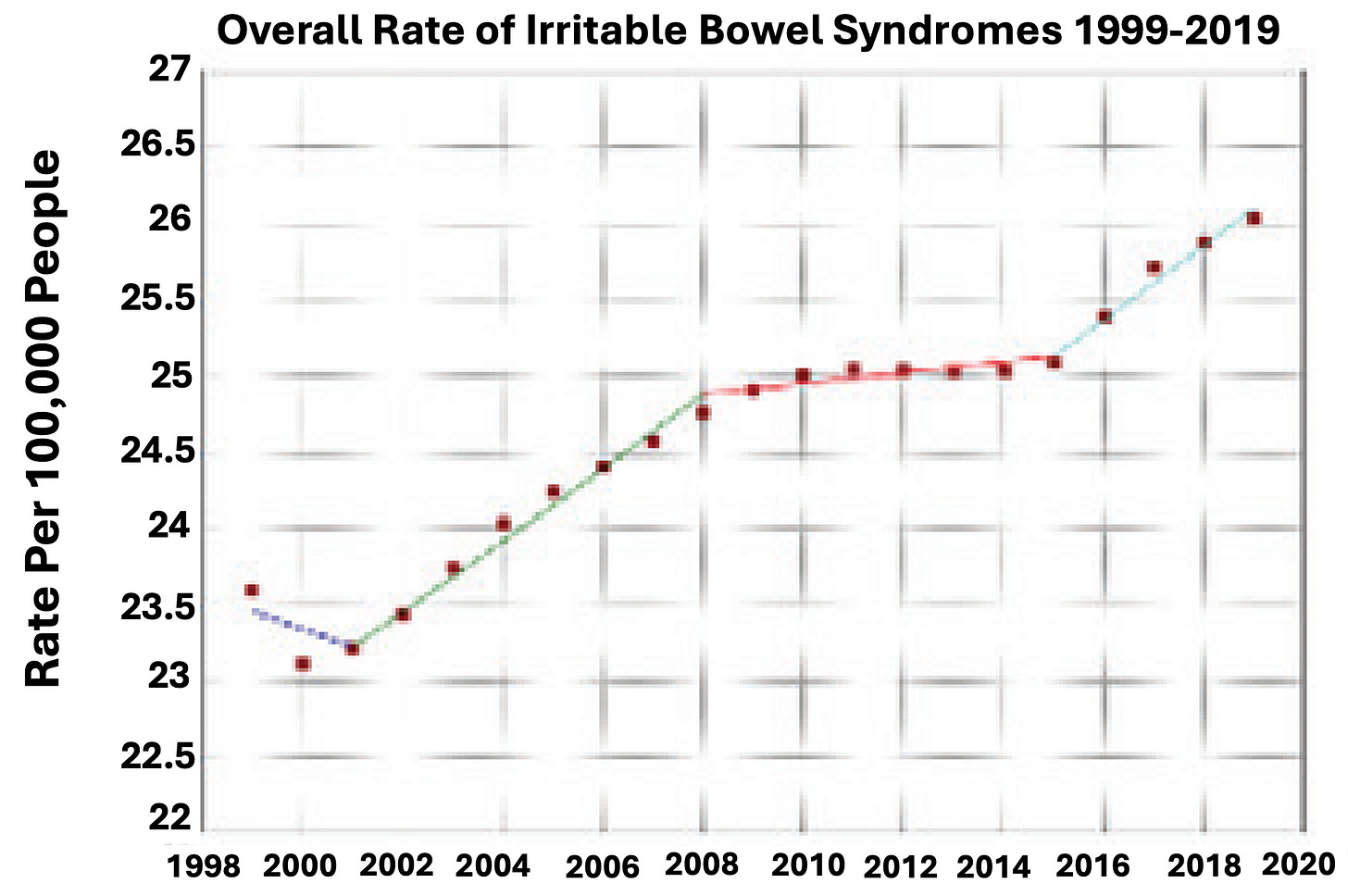
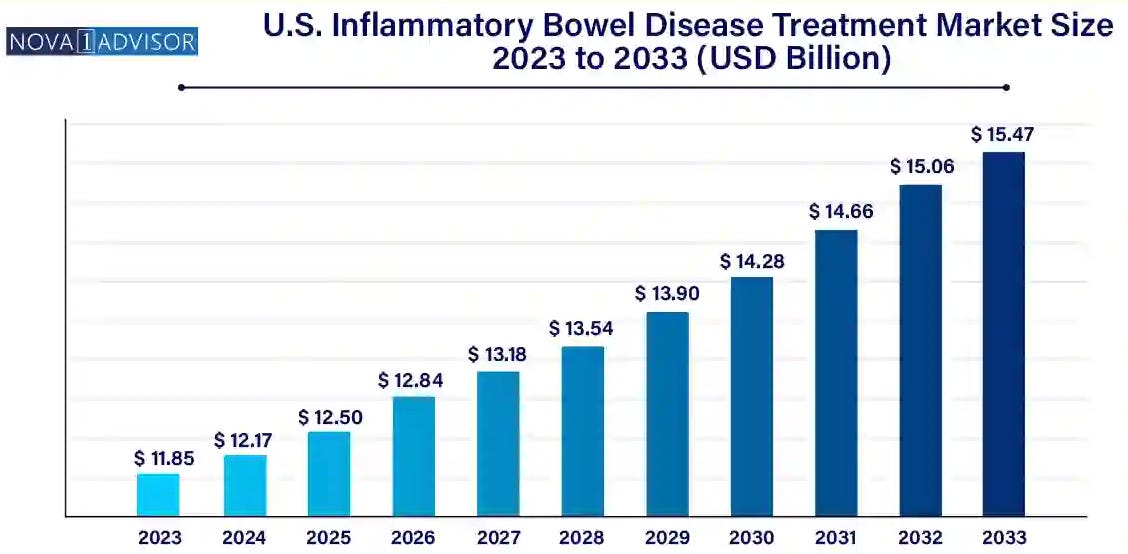
I would argue the situation with inflammatory bowel diseases (which affect approximately 1.17% of adults) is quite similar, as the rate of it keeps increasing. Yet, no one knows what causes it, allowing a costly status quo to perpetuate (where patients have no option except to spend thousands each year on the IBD drugs).
As such, this greatly disincentivizes research into the actual causes of them (e.g., specific pesticides and herbicides—like glyphosate—have been repeatedly linked to IBD—as have junk food diets1,2,3 and food allergies1,2). Likewise, we’ve seen numerous children who get their meningococcal vaccine for college develop Crohn’s disease but never seen this link be discussed—which may, in part, be due to Wakefield’s infamous 1998 paper showing that children who developed autism after the MMR had significant inflammatory bowel diseases (along with three earlier ones linking the measles vaccine virus to IBD1,2,3) making this topic be taboo to research further (despite numerous therapies being discovered which were able to improve autism by reducing bowel inflammation).
Note: the only research I know of on this topic was a large survey Steve Kirsch conducted, which found vaccinated children were 3.5X more likely to develop Crohn’s disease.
Likewise, one of the most common side effects of the COVID vaccines was an exacerbation of a pre-existing autoimmune disorder (e.g., an Israeli government study which found that 24.2% of those receiving a booster developed an exacerbation of a pre-existing autoimmune condition), and throughout the vaccine campaign, I saw numerous cases where this happened with IBD (including cases where vaccine supporting medical students and physicians acknowledged their issues were likely due the vaccine).
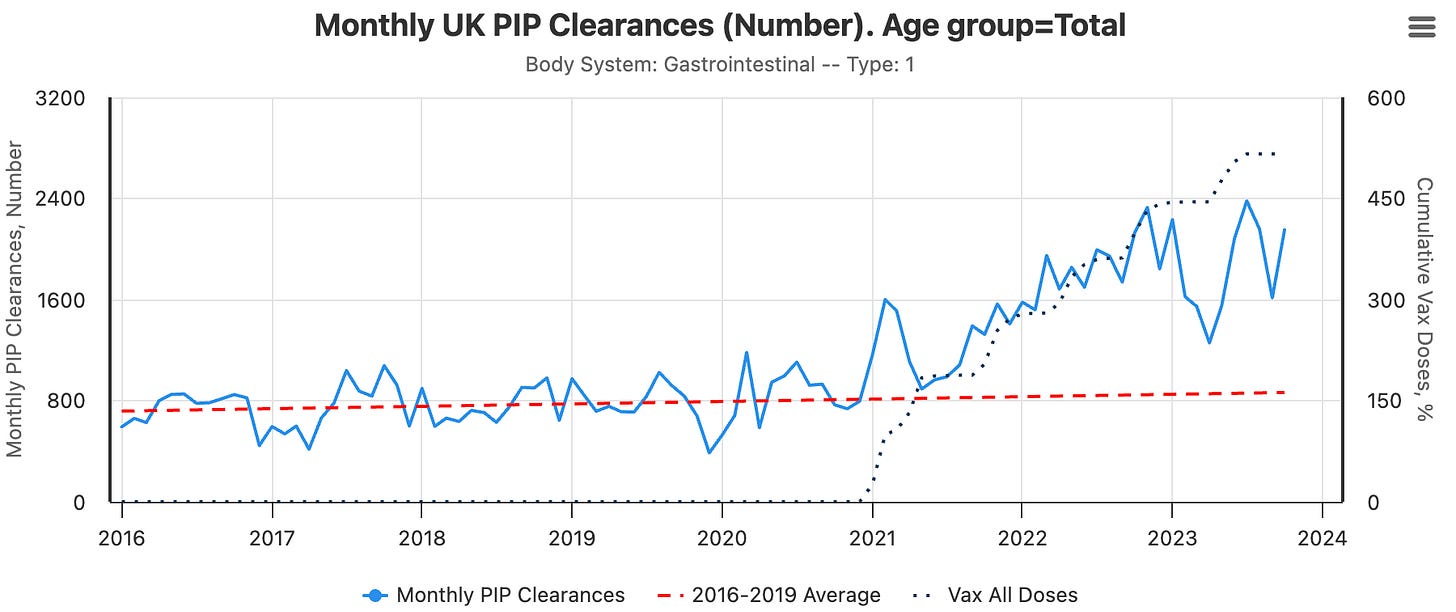
Note: the more severe a reaction is to a pharmaceutical, the rarer it is, and as such, the COVID vaccines disabled far more than they killed. While investigating the economic cost of the COVID vaccines, Ed Dowd’s team made the horrific discovery that the vaccines caused a massive spike in disability in America (16% more Americans are now disabled than they were at the start of COVID)—and this increase shows no signs of stopping (it’s actually beginning to accelerate). The above chart came from their investigation of England’s disability data (and virtually mirrors England’s increase in disability for immunological diseases).
Finally, as severe illnesses are rarer than mild ones, a much larger portion of adults are affected by chronic gut inflammation (e.g., 6.1% of Americans have irritable bowel syndrome)—with many of these disorders (e.g., leaky gut syndrome or moderate gluten sensitivity) being either understudied or outright dismissed by the medical system.
Note: we find irritable bowel disorders are frequently missed (e.g., because the scopes gastroenterologists use don’t reach much of the small intestine, and capsule endoscopies, which can do so are rarely used now). As IBD often occurs concurrently with rheumatologic disorders (particularly spondyloarthropathies), and many rheumatologic medications make IBD worse, it is often quite helpful to screen those patients for an antibody test for Crohn’s beforehand, and if positive, give them a rheumatologic drug that improves rather than worsens IBD—all of which is discussed further in this article on natural and pharmaceutical treatments for autoimmune disorders.
As such, while reviewing the literature on DMSO, I was immediately struck by the rapid and dramatic IBD improvements reported in many cases. These reports included diagnostic testing confirming complete remission of Crohn’s disease or ulcerative colitis, consistent and rapid relief of the colicky pain commonly associated with IBD, and successful treatment of an intermittent, severe colonic paralysis following colon cancer surgery alongside progressing scleroderma. Several authors specifically noted that IBD responded exceptionally well to DMSO—something one reader here also observed in their own ulcerative colitis patients.
Likewise, I periodically have exchanges like this (which I was given permission to share):
Hi! I’m desperately hoping you can help me. How would I take DMSO to help a diverticulitis flare up? Thank you so so much! I don’t trust anyone else but you!
I wrote a quick reply 19 minutes later, and then two hours and 12 minutes later received this reply.
Thank you from the bottom of my heart!!! You saved me.
Then, I asked how fast the response was:
It actually helped a lot very quickly!! I think taking it really helped to decrease the pain and inflammation.
I was ready to go to the hospital! Thank you again from the bottom of my heart!
Note: since I receive dozens of correspondences each day, I can't respond to most of them. For this reason, I maintain monthly open threads where readers can ask any lingering questions from the previous month, and everyone else can also view the answers. Likewise, I try to answer all the questions I expect to arise in each article (e.g., 95% of the DMSO questions I receive are answered within the articles) or write new ones to address recurring questions I receive (e.g., how do you use DMSO for gastrointestinal disorders).
Umbrella Remedies
Given that DMSO is primarily thought of as a pain treatment (due to the rapid and dramatic improvement it frequently produces), it seems quite surprising that it could also create the profound bowel benefits described above. However, in medicine, there are a few therapies (e.g., ultraviolet blood irradiation) that have the ability to cure a wide range of diseases, and as such are referred to as “umbrella therapies.” This is because, rather than targeting a specific molecular receptor, they can address the root causes of many illnesses, such as poor circulation throughout the body, inflammation, and cells entering a state of shock where they stop functioning and eventually die.
DMSO does that, and in turn, has repeatedly been shown to be remarkably effective for a wide range of disorders including:
- Strokes, paralysis, a wide range of neurological disorders (e.g., Down Syndrome and dementia), and many circulatory disorders (e.g., Raynaud’s, varicose veins, hemorrhoids), which I discussed here.
- A wide range of tissue injuries, such as sprains, concussions, burns, surgical incisions, and spinal cord injuries (discussed here).
- Chronic pain (e.g., from a bad disc, bursitis, arthritis, or complex regional pain syndrome), which I discussed here.
- A wide range of autoimmune, protein, and contractile disorders, such as scleroderma, amyloidosis, and interstitial cystitis (discussed here).
- A variety of head conditions, such as tinnitus, vision loss, dental problems, and sinusitis (discussed here).
- A wide range of internal organ diseases, such as pancreatitis, infertility, COPD, and endometriosis (discussed here).
- A wide range of skin conditions, such as burns, varicose veins, acne, hair loss, ulcers, skin cancer, and many autoimmune dermatologic diseases (discussed here).
- Many challenging infectious conditions, including chronic bacterial infections, herpes, and shingles (discussed here).
- Many aspects of cancer (e.g., many of cancer’s debilitating symptoms, making cancer treatments more potent, greatly reducing the toxicity of conventional therapies, and turning cancer cells back into normal cells), which I discussed here.
Note: most of the above have also been shown for ultraviolet blood irradiation. Likewise, similar data exists for ozone, another umbrella remedy that I plan to focus on once the DMSO series is finished.
Additionally, DMSO possesses a unique ability to enhance the absorption and potency of pharmaceutical medications and natural therapies by facilitating their passage into the body. This property has transformed the way conventional and natural medicine is practiced, opening up nearly limitless possibilities for incredible therapeutic combinations (discussed here and here), and most importantly, DMSO is extremely safe (provided it's used correctly).
As such, a wealth of data (detailed in the above articles) has accumulated, showing DMSO has a high rate of efficacy in a wide range of conditions. Since DMSO was widely available, it quickly spread like wildfire across America in the 1960s (particularly due to how rapidly it alleviated “incurable” pain). Regrettably, the FDA then stepped in and went to war with DMSO to protect the status quo. In the decades that followed, despite the public, the scientific community, and Congress petitioning the FDA to rescind their prohibition on DMSO, it all fell on deaf ears (all of which I chronicled here).
Eventually, the 1994 DSHEA Act (passed in response to public outrage over the FDA raiding supplement providers at gunpoint) simply took away the FDA’s ability to regulate natural medicines, and DMSO was able to re-enter the marketplace. Sadly by this time, despite thousands of studies supporting its use, many American pharmaceutical products using DMSO and it being widely used outside the United States, DMSO had become yet another forgotten side of medicine.
As what they did to DMSO has always really bothered me (particularly due to its ability to rescue people from a life of debility after strokes or spinal cord injuries), I decided to try publicizing it and do all that I could to give a strong case for its use. Fortunately, numerous readers here were willing to try it, bringing it to public consciousness, and much like the 1960s (when it first emerged) it again has rapidly caught on.
In turn, I've received numerous testimonials from readers around the world about the life-changing effects DMSO has had on them. Recognizing the importance of not letting these stories become forgotten, I’ve devoted a significant amount of time to compiling those I came across here—which has now totaled to over 3,000 reports of DMSO treating a wide range of conditions.
The majority of those testimonials align with the well-recognized functions of DMSO, but at the same time, I’ve received many astonishing ones, such as the diverticulitis example above. As such, this article will focus on exactly what the data shows DMSO does for the gastrointestinal system, and how many reader reports mirror what is displayed within those studies.
Note: one of DMSO’s key anticancer properties is that it causes cancer cells to differentiate (transform) into normal cells. Data also shows it can create this effect in stem cells1,2,3 and hence produce the cells needed to regenerate a damaged organ (e.g., this has been repeatedly demonstrated for the heart1,2,3,4,5,6 and kidneys1).
Stomach
I adore your substance. Your suggestion to try oral DMSO to heal my stomach issues [and my gut] is slowly but surely working. I have been seeing various docs about the issue for over 2 years now- and your suggestion was the first one to actually help! — from a retired M.D.
DMSO has been repeatedly shown to heal the stomach, stop life-threatening bleeds and modulate its function, particularly when injuries follow excess acidity:
•A study of 138 patients with chronic gastritis (stomach inflammation), duodenal ulcers (mostly in remission), or one gastric ulcer found that 50% DMSO applications to the epigastric area often reduced gastric juice volume and acidity in those with duodenal ulcers and hypersecretion, and enhanced antral mucosa neutralization in some with acidic conditions. In chronic gastritis with preserved acid secretion, the effects of DMSO varied (no change, reduced, or slightly increased secretion and acidity). In secretory insufficiency, DMSO had no stimulating effect, either unchanged or slightly reduced secretion. In short, DMSO consistently normalized excessive stomach acid production.
I have been drinking DMSO diluted in water daily for about 3 months with no known side effects…Since starting this pattern my reflux has disappeared and I am feeling great.
•In lab tests, 9% DMSO increased pepsin enzyme activity by 83.4%, lowered the Km value to 1.50 mg/mL, and altered pepsin’s molecular conformation without inhibiting aromatic amino acid absorption—hence making pepsin more effective at digesting protein.
Bleeding ulcers in the stomach and duodenum remain a major issue in medicine, with roughly 10,000 Americans dying annually from them, and around 10 billion dollars are spent each year on them. As such, DMSO’s ability to treat and prevent them is quite noteworthy:
•In 115 hospitalized patients with pelvic fractures or hypovolemic shock at risk for stress-induced gastric ulcers, 22% of 58 controls developed ulcers, compared to only 4% of 57 receiving DMSO and 3% of 62 receiving allopurinol. Notably, none of the DMSO-treated patients deteriorated or required emergency surgery, whereas 8 controls and 1 allopurinol recipient did, with 3 control patients dying.
•In 101 patients with hematemesis (coughing up blood) due to erosive gastritis, oral DMSO and allopurinol (administered every 6 hours for 5 days) resulted in 8% having further hematemesis episodes, and 9% having endoscopies showing hemorrhagic inflammation. In contrast, 29% of untreated controls had further hematemesis episodes, and 44% showed hemorrhagic inflammation. No treated patients required surgery, while three controls did, with one death.
•In 58 patients with NSAID-induced erosive gastritis, DMSO reduced re-bleeding, stabilized hemodynamics, and promoted gastric erosion healing (7% had erosions at 48 hours) compared to placebo (50% of 59 patients), with fewer patients requiring transfusions or surgery.
•In 40 patients with multiple fractures and hemorrhagic shock, DMSO reduced stress-induced acute gastric mucosal injury incidence to 2.5% (1/40) compared to 23.8% (10/42) with placebo, with fewer requiring surgery.
•In rats with corrosive esophageal burns, intraperitoneal DMSO reduced stricture formation by decreasing malondialdehyde, nitric oxide, tumor necrosis factor-alpha, and interleukin-6 levels, lowering the stenosis index and histopathologic damage scores compared to controls.
•In rats, DMSO significantly accelerated healing of reserpine- and 5-hydroxytryptamine-induced acute ischemic gastric mucosal injury, reducing injury severity over 4 days compared to placebo.
•In three separate placebo controlled rat studies, DMSO at (1%, 2%, and 5%) demonstrated significant protection from a variety of injuries to the stomach lining in a dose dependent manner. In the first, 2 days of DMSO pretreatment counteracted ischemic injuries (from reserpine or serotonin) to the gastric mucosa, with 1% DMSO reducing the injury area, 2% protecting 60-80% of the stomach (depending on the injuring agent used), and 5% fully preventing it. In the second study, DMSO prevented ethanol (alcohol) from damaging the stomach, with 1% reducing injury in 70% of rats, while 2% and 5% eliminated it entirely. In the third, 1% DMSO reducing stomach ulceration by 40%, 2% by 80% and 5% by 100% (providing complete protection).
•DMSO (2 or 5% solutions) completely protected rats against aspirin-induced gastric mucosal injury (0% incidence vs. 30% without pyloric ligation and 80% with ligation in placebo) and ethanol-induced injury (0% incidence vs. 100% in placebo), without affecting H+ output.
•In rats subjected to water-immersion stress, DMSO inhibited gastric ulcer formation. Similarly, in rats with cold-restraint stress, DMSO, allopurinol, or their combination significantly reduced lipid peroxidation and stress-induced gastric and lung injuries compared to saline controls.
Note: other studies have also shown DMSO protects against gastric stress ulceration.
Other data also corroborates DMSO’s ability to heal severe gastric conditions and support recovery in challenging cases:
•A 1968 patent application reported oral DMSO effectively treated gastrointestinal conditions: 28 patients with acute gastritis resumed work within 5–8 days, free of nausea, vomiting, and pain, with 21 remaining symptom-free after one year; 13 patients with chronic gastritis improved after 1–2 months and stayed relapse-free for a year with periodic retreatment; 5 patients with recent peptic ulcers were cured without recurrence over a year; 6 patients with enterocolitis improved after 8 days and returned to work within 2 months; and 3 patients with mucomembranous colitis were cured after 3 weeks.
•In patients with refractory gastric and duodenal ulcers unresponsive to three months of cimetidine and one month of bismuth chelate, oral DMSO achieved complete healing within four weeks with no significant side effects, compared to placebo.
•In 126 patients with healed duodenal ulcers and Helicobacter pylori infection, oral DMSO reduced one-year ulcer relapse to 6%, compared to 47% with placebo and 24% with cimetidine, showing superior efficacy. No comparison between DMSO alone and DMSO with allopurinol was reported.
•In 12 patients with refractory peptic ulcers (eight duodenal, four gastric), oral DMSO achieved complete healing within four weeks, compared to placebo.
Finally, DMSO has also been shown to alter other characteristics of the stomach (e.g., it made the stomach more transparent, increasing light transmittance by 29%; it increased the stomach’s sensitivity to vagal stimulation; and at concentrations above 50%, it decreased stomach acid secretion in a dose-dependent manner).
Note: Numerous key human studies cited in this section and the next (where DMSO was often administered orally with a nasogastric tube) were conducted by a DMSO researcher in Iraq between 1990–1994, during a period when its medical system was robust before economic sanctions and conflicts disrupted Iraq’s healthcare infrastructure, a pattern also observed in Libya post-NATO intervention (where pivotal DMSO research was also previously conducted)..
Intestines
I’ve used DMSO for Crohn’s since 2012. Pure miracle for Crohn’s.
Numerous studies have explored DMSO’s interactions with the small and large intestines. For example, autoradiography in mice showed that radiolabeled DMSO selectively accumulates in the large intestinal mucosa, which may help explain its notable effectiveness in treating bowel inflammation. Additionally:
•Despite being an acetylcholinesterase inhibitor (and hence parasympathetic activator), DMSO (0.2-1.4%) contacting the intestines does not promote peristalsis (which is fortunate as otherwise diarrhea would be a frequent side effect of oral DMSO use). Conversely, another study (of pig intestines) found DMSO was a nonspecific antagonist of carbachol, histamine, and nicotine on isolated guinea pig ileum (all of trigger peristalsis).
•DMSO at low concentration (e.g., between 0.16%-5%) typically did not affect intestinal permeability or the gut absorption of other substances.1,2,3,4 However, in certain circumstances it did (e.g., if high amounts of glucose or galactose were present DMSO increased their absorption by allowing them to directly diffuse through the intestines and at DMSO concentrations above 0.3M it reduced intestinal absorption of amino acids with completion seen at 1M).
Note: assuming a DMSO mixture gets diluted by 50% once it is mixed with the stomach and intestinal fluids, the typically recommend oral dose results in an intestinal DMSO concentration roughly half the 0.3M threshold identified in that study (although I suspect it’s actually lower since of the DMSO will diffuse directly into the body as it travels through the digestive tract).
DMSO’s protective properties shield the bowels from a variety of serious injuries. For example, cutting off the blood supply to the small intestine will rapidly cause the tissue there to die and often rupture (leading to fatal peritonitis). However, DMSO has been repeatedly shown to prevent this severe illness:
•In rats, giving IV DMSO to rats after 30-60 minutes of their entire intestinal blood supply being cut off (or 150 minutes of one section’s blood supply being cut off), resulted in 28 out of 29 not developing gangrene, and within 24 hours, there was no evidence of ischemic damage to the intestines. Similar results were obtained in a 1985 study (which also noted significantly reduced inflammation and adhesions) and a 2016 study which showed greater tissue protection with higher DMSO doses (along with it stabilizing blood pressure and improving metabolic status).
•In horses, DMSO has been shown to prevent intestinal ischemia-reperfusion injuries (particularly within the jejunum or ascending colon) and to reduce intestinal microvascular permeability, edema, inflammation, and bowel-to-bowel adhesions.1,2,3,4,5,6
•Similar results have also been seen in other animals such as dogs or calves (e.g., one study found DMSO significantly improved pH, PCO₂, PO₂, O₂ saturation, and peritoneal fluid lactic acid levels).1,2,3,4
Additionally:
•In rats, oral DMSO (1%, 5%, or 10% solutions) provided dose-dependent protection against acute and chronic duodenal ulceration, reducing incidence to 80%, 30%, or 30% in acute cases and 40%, 20%, or 20% in chronic cases compared to 100% in placebo groups.
•In rats, DMSO and allopurinol reduced acute duodenal ulceration incidence to 70% at 2 days, 30% at 5 days, and 0% at 7 days (vs. 100%, 80%, and 50% with placebo) and chronic duodenal ulceration to 80% at 5 days, 30% at 10 days, and 10% at 15 days (vs. 100%, 90%, and 80% with placebo).
•DMSO has been observed to reduce intestinal cell death in jaundiced rats (following bile duct ligation).
DMSO’s protective properties have also been shown to protect the intestines from other lethal stressors:
•In rats with 20% third-degree burns, compared to placebo, DMSO solution applied to the mesentery reduced white blood cell adhesion in microveins, improved microcirculation, and preserved immune-active white cells.
Note: blood sludging is a common consequence of severe burns that likely triggers many of the systemic complications they create.
•In dogs, oral DMSO improved survival by 75% against 12.5 Gy (a lethal dose) of abdominal radiation and prevented radiation-induced intestinal damage.
•DMSO (a widely used cryopreservant) has been shown to protect intestinal segments in dogs from necrosis following cryoinjury (dying after being frozen).
In addition to protecting intestinal tissue from injury, DMSO has also been shown to heal them:
•A study randomized 302 consecutive patients with previous symptomatic duodenal ulceration that was shown to have healed, and who were smokers and social drinkers, to receive four different treatments. Of the 220 available for evaluation, 65% of those who received a placebo had a recurrence of the ulcer, 30% of those who received cimetidine did, while only 13% of those who received oral DMSO did.
•Another author reported on a doctor who had 5 patients with recurrent duodenal ulcers and were social drinkers he gave DMSO to. They were examined once a month for a year, and all 5 had no recurrence of ulcer symptoms (along with having better health than expected and excellent attendance at work). He also highlighted the case of a 55 year old woman with severe digestive tract issues (e.g., internal bleeding leading to her being anemic with a hemoglobin of 5.0), weakness, fainting and shortness of breath. After receiving an emergent blood transfusion and being diagnosed with angiodysplasia in her GI tract, she was started on IV iron (which is not pleasant and did not help her, causing her to progress to being terminal). She was then started on injected DMSO and B-12, recovered, and over the six years of follow-up, did not require any subsequent blood transfusions.
•In a patient with refractory duodenal ulceration unresponsive to three months of cimetidine and one month of bismuth chelate, oral DMSO achieved complete ulcer healing within four weeks, compared to no improvement with placebo
Note: this type of chronic internal bleeding is quite challenging to treat (e.g., the only other approach I know of that consistently helps here is a Chinese herbal formula).
•A randomized double-blind study of 363 consecutive patients whose duodenal ulcers did not heal despite 3 months of treatment with cimetidine (and who were cigarette smokers or social drinkers), were given either cimetidine twice a day alone or with DMSO or allopurinol. In 315 evaluable patients, at 8 weeks, 60% of those who received cimetidine recovered, whereas 100% of those who received DMSO recovered. Additionally, the one year relapse rate was 29% for cimetidine alone, 8% for those who took allopurinol, and 7% for those who took DMSO.
Note: another study used DMSO in combination with electrophoresis (to direct DMSO to the ulcer) to treat peptic and duodenal ulcers.
•A randomized double-blind study took 238 patients with symptomatic acute duodenal ulceration who were smokers and social drinkers, and were randomized to receive for 8 weeks cimetidine or 8 weeks of a half dose of cimetidine plus oral DMSO (400mg two times a day) or allopurinol. After 8 weeks, 69 of the 87 (79%) who only received cimetidine recovered, whereas 100% of the 85 who received DMSO did. Additionally, 67% of those who received cimetidine over the next year relapsed, compared to 6% of those who also took DMSO.1,2
•In rats where part of the colon had been removed (requiring each remaining end to be surgically stitched together), a DMSO quercetin mixture given intraperitoneally post surgery significantly improved healing (e.g., the maximum strength of the sutured tissue along with hydroxyproline, malondialdehyde, superoxide dismutase, and catalyze levels had a 1.4-3.9 fold improvement).
Note: many studies show DMSO significantly improves healing from surgery and heals chronic wounds.
•A Russian suppository containing (50%) DMSO and hyaluronic acid (along with vitamin C, collagen, and coenzyme Q10) was developed to treat rectal fissures.
Note: the gastrointestinal tract appears to be more sensitive to DMSO than most parts of the body, and in some of the studies I reviewed, DMSO could injure its gastrointestinal lining. As injuries like those suggested by the studies are never reported in practice, I believe those results were due to significantly higher concentrations of DMSO contacting the gastrointestinal lining than are seen following typical oral consumption (much in the same way, as mentioned above, DMSO can inhibit the absorption of amino acids, but in practice parents around the world have found the combination of two is profoundly transformation for developmental delays and Down Syndrome). In my eyes, all of this strongly argues for avoiding higher oral DMSO doses than those typically used by the DMSO community.
DMSO’s anti-inflammatory properties (and histamine receptor antagonism) have also been repeatedly shown to treat inflammatory bowel diseases:
•A double-blind, randomized study evaluated patients with recurrent attacks of proctosigmoidal ulcerative colitis that were not being prevented by their prophylactic medical regimen, three different combinations of standard therapies, or a standard treatment with DMSO (46) or allopurinol (45). After two weeks, 51% of those treated with a standard regimen (sulfasalazine or prednisolone) recovered, while 84% of those using DMSO or allopurinol recovered. Over the next year, those treatments were continued, and it was observed that the standard treatment (sulfasalazine) had a 25% relapse rate. In contrast, that rate was only 5% of those taking DMSO or allopurinol.
•In mice with encapsulating peritoneal sclerosis (EPS), a severe complication of peritoneal dialysis that leads to intestinal obstruction with or without peritonitis, DMSO treatment reduced parietal and visceral peritoneum thickening by 30% compared to controls. It also decreased CD4, CD8, and IFN-γ-producing T cells and Ascites cytokines (IFN-γ, IL-17a, TNF-α, IL-23) while increasing IL-4, IL-10, CD69 T cells, and Treg cell differentiation—all of which reduce inflammation. Finally, these results were corroborated by using DMSO to differentiate Treg cells in a test tube, and once those cells were implanted in mice, they also prevented EPS.
Note: DMSO has also been used to treat ascites in hamsters with melanoma.
DMSO and the carnivore diet worked for me for Irritable Bowel Syndrome and Interstitial Cystitis.
•Amyloidosis (the deposition of irregular proteins that clump together) is frequently seen alongside autoimmune disorders. As DMSO stabilizes and solubilizes proteins, it effectively treats amyloidosis, and due to the lack of effective treatments for amyloidosis, many studies have been conducted demonstrating DMSO’s utility for amyloidosis (listed here). These include cases where amyloid deposition had been causing severe gastrointestinal issues, which fully resolved following DMSO,1,2,3 including cases that would have otherwise been fatal.
•In one report, daily oral DMSO successfully treated 10 out of 15 patients with AA amyloidosis linked to autoimmune disease; notably, all 4 cases related to Crohn’s disease achieved full remission. Among the 6 patients presenting with gastrointestinal symptoms, all experienced resolution of diarrhea and protein-losing gastroenteropathy—with no serious adverse effects reported.
Note: in another report, a 1.2 by 1.2 cm and a 1.0 by 1.2 cm gastric lesion from localized amyloidosis completely resolved following oral DMSO taken three times a day.
•Intraperitoneal injections of zymosan trigger are used to trigger systemic inflammation akin to sepsis. In two separate rat studies, compared to placebo, DMSO was shown to reduce inflammation, preserve intestinal blood flow, and prevent damage to the gut and intestinal lining (a significant issue in both chronic and subtle inflammatory bowel disorders).1,2
•In a third similar study, subcutaneous DMSO given one hour after zymosan increased 24-hour survival from 55% to 90%, reduced liver, kidney, and intestinal swelling by 10-20%, lowered inflammatory markers (TNF-α, IL-6) by 20-30%, and improved organ blood flow and tissue damage
Likewise, in numerous animals, intraperitoneal DMSO has also been repeatedly found to improve peritonitis, including purulent or diffused cases,1,2,3,4,5,6,7As DMSO potentiates antibiotics, some of those studies used a combination (e.g., DMSO and kanamycin) to successfully treat peritonitis,1,2 while others found DMSO altered abdominal antibiotic absorption, caused antibiotics to concentrate in the peritoneum and increased bacterial sensitivity to them.1,2,3
Note: under standard hospital care, peritonitis kills 13.16% of patients under 50 years and 33.33% of patients over 50 years—making the improvements seen with DMSO quite profound.
DMSO has also been combined with antibiotics to treat abdominal abscesses, and at concentrations comparable to those oral DMSO will reach in the intestine, inhibit the growth of many common gastrointestinal pathogens (e.g., Escherichia coli, Shigella dysenteriae, Candida albicans).1,2
Note: the DMSO community has also reported success treating SIBO (small bacterial bowel overgrowth) and leaky gut syndrome with DMSO.
Similarly, in a feline case of viral enteritis (likely caused by panleukopenia), DMSO induced a clinical improvement, again indicating both DMSO’s antimicrobial properties and protective effects on gastric and intestinal lining.1,2
Finally, since DMSO treats the whole body rather than one specific issue, individuals will often observe it treat other illnesses (e.g., DMSO began being used to treat macular degeneration after participants in pain trials reported their lost vision returning):
I had a severe case of plantar fasciitis that made it difficult to walk. For 1.5 years, I did stretches, exercises, wore a brace, etc. Nothing helped. Within two weeks [of topical DMSO], I could put weight on my foot again. Within a month, I could walk almost normally. In two months, there were days when my foot was not in pain at all..I am [now] up to 6,000 steps a day.
Once my foot was on the mend, I started to take DMSO internally. I have mild ulcerative colitis. Since I've been taking DMSO, I've only had one episode of bleeding, and it resolved in two days. (Normally, the healing takes weeks.) And I typically suffer from sinus headaches caused by allergies…Since I've been taking DMSO internally, I have only had one sinus headache.
Liver and Gallbladder
DMSO has also shown great promise for protecting the liver and addressing issues with the biliary (bile) tract
Liver Injury and Protection:
•In rats exposed to chloroform or bromobenzene, DMSO administered 24 hours post-exposure was found by multiple studies to reduce plasma ALT levels significantly, limit centrilobular liver lesions, restore sinusoidal perfusion, reduce leukocyte adhesion, and modify Kupffer cell phagocytic activity (mitigating the hepatic inflammatory response), and prevent chloroform-induced kidney necrosis. Delaying treatment beyond 24 hours led to a loss of protection, with progression to bridging necrosis and elevated ALT, emphasizing DMSO’s dose- and time-sensitive hepatoprotective effects.1,2,3,4
•In F344 rats subjected to warm ischemia as non-heart-beating donors, DMSO (2–6 ml/kg, ip) preserved liver and kidney viability, maintaining potassium and LDH levels comparable to non-ischemic controls.
•A study found that giving DMSO to rats 10 hours after they were exposed to halothane (an inhaled anesthetic that was phased out of the more affluent nations due to its toxicity profile), chloroform, or bromobenzene, prevents liver and kidney damage that these toxicants typically cause. A follow-up study, instead administered DMSO 24 hours later, found DMSO reduced the resulting liver damage 4-fold (which without treatment within 48 hours would have occupied 40-50% of the liver) and ALT levels 8-16 fold.
Note: this study also found DMS (a DMSO metabolite) offered no protective effects.
•In rats exposed to thioacetamide, DMSO reduced liver and brain oxidative stress, lowered liver enzymes (AST, ALT, LDH), decreased hyperammonemia, and increased BUN levels, mitigating lipid peroxidation and preserving glutathione and catalase activity. Similar results were found in another study.
•In rats, daily oral DMSO for 4 weeks was seen to prevent dimethylnitrosamine induced liver damage without any major side effects. Specifically, it prevented body and liver weight loss and the induction of hepatic fibrosis and the expression of mRNA for type-1 collagen in the liver. Additionally, DMSO was also found to inhibit LPS-induced TNF-alpha and nitric oxide production (e.g., TNF-alpha mRNA levels were reduced).
•In rabbits subjected to portal vein or hepatic artery clamping, DMSO in a dose-dependent manner has been repeatedly found to reduce ischemic and ischemia-reperfusion liver damage and oxidative stress.1,2,3,4,5,6,7
•A Brazilian study found that DMSO reduced the oxidative stress that followed part of the liver being surgically removed.
•In primary cultured rat hepatocytes exposed to Tylenol, DMSO reduced toxicity by preserving plasma membrane integrity, restoring glutathione to ~63% of normal levels, and preventing cytosolic free calcium elevation. A second study also found that DMSO prevented this liver damage, while a third study found that DMSO prevented liver damage, but in the presence of natural killers, it could instead increase it.
•DMSO administered to Syrian golden hamsters reduced the incidence and severity of Tylenol-induced hepatocellular injury, attenuating increases in serum glutamic-pyruvic transaminase and alkaline phosphatase activities, indicating a protective effect against liver toxicity.
•A rat study found DMSO inhibited liver necrosis and oxidative stress triggered by injecting D-Galactosamine and restored liver vitamin C levels.
•In galactosamine-sensitized mice, DMSO (10 mL/kg) inhibited endotoxin-induced hepatic NF-κB activation, reduced plasma TNF-α by 86%, suppressed ICAM-1 mRNA, decreased neutrophil accumulation by 79%, and reduced liver injury by 80%.
•DMSO was shown to protect liver, heart, and airway cells by inhibiting caspase proteins (reducing cell death).
•DMSO was found to inhibit the NF-kappa B activation, ICAM-1 gene transcription and TNF-α formation which following endotoxin exposure, thereby preventing liver injury.1,2
•A rat study found DMSO inhibited lipid peroxidation in hepatocytes triggered by carbon tetrachloride and improved the antioxidant system’s state. Likewise, a rabbit study found that DMSO and tocopherol prevented the liver damage caused by injecting carbon tetrachloride. Finally, a third liver study found DMO and alpha-tocopherol counteracted the oxidative damage caused by chemical injury.
•In primary cultured rat hepatocytes, 2% DMSO with collagen-coated dishes extended cell survival to 96 hours (vs. 48 hours for controls), maintained 86% cell viability at 96 hours and 78% at 120 hours, preserved cell shape, doubled glycogen content, and retained 50–60% cytochrome P450 content.
•DMSO was repeatedly shown to cause mesenchymal stem cells to differentiate into liver cells, potentially explaining how DMSO is able to regenerate the liver.1,2
•In isolated rat hepatocytes, DMSO and 2% and 8% DMSO caused a biphasic inhibition of sympathetic stimulation of liver cells. Likewise, DMSO was observed to permeate isolated rat hepatocytes, but its ability to do so decreased at higher concentrations.
•In primary cultured rat hepatocytes, DMSO with collagen-coated dishes extended cell survival, maintained high cell viability, preserved cell shape, doubled glycogen content, and retained cytochrome P450 content
•In Chang liver cells, 0.1% DMSO increased CYP3A4 mRNA and protein expression, while 0.01%–0.05% DMSO increased CYP3A4 protein only; combined with testosterone or rifampicin, DMSO enhanced CYP3A4 and CYP2C9 protein expression.
Liver Failure
•One author reported on a study with 12 patients who had terminal liver cirrhosis who agreed to stop drinking all alcohol for the duration of the program were put on daily oral DMSO and aloe vera. Of the 8 who chose to continue the program for 6 months, all had improved health, significantly reduced vomiting, and improved liver function tests, and rather than all being dead within one year as expected, they were in better condition than they had been at the start of the study.
Note: if using DMSO for cirrhosis, it is critical to stop consuming alcohol, as DMSO can slow the metabolism of alcohol.
Other Protective Effects
•In mice exposed to lethal radiation (9.0–9.5 Gy), oral DMSO (10 g/kg) given 15 minutes to 4 hours prior achieved 100% survival, enhanced bone marrow and intestinal stem cell regeneration, reduced blood cell loss, and mitigated liver and other organ damage.
•In rats exposed to carbon monoxide, DMSO reduced brain and cardiac ischemic injury, lowering cerebral neuronal alteration, degenerative neuron rates, and cardiac injury scores after one day. Combined with ethyl pyruvate, DMSO reduced hepatic injury scores and further reduced cardiac.
Gallbladder and Biliary System
Multiple readers have reported remarkable results with DMSO for cholecystitis:
IV DMSO saved my gallbladder and instantaneously reduced my inflammation to almost nothing in 2013.
I found out a couple of months ago that I have gallstones and was basically told I couldn’t do anything about it. One more holistic dr gave me a supplement from Amazon to try to reduce them, and I took it religiously [but it didn’t work]. My right side then starting hurting, feeling like muscle soreness. It went on for a couple weeks [after which] I started poking around my side one evening and got pain/pressure in my right shoulder blade afterwards and knew then it was my gallbladder.
I immediately looked up your articles and ordered some DMSO. Since I started applying it a week or two ago, the pain and symptoms have almost completely gone away. I am working with a functional Dr now to get to the bottom of everything, and have an ultrasound scheduled for tomorrow, but it has helped me tremendously, not just with the minimal pain, but also just peace of mind as I was terrified of the after effects of what felt like an unavoidable cholecystectomy.
Data also supports DMSO treating complications of the bile ducts and gallbladder:
• A rat study created obstructive jaundice by ligating the common bile ducts and found that DMSO mitigated pathologic effects (e.g., normalized laboratory values). Another rat study found DMSO protected intestinal cells from dying after bile duct ligation.1,2
•Injecting 90% DMSO mixed with 5% hexametaphosphate into the biliary tract was found to effectively dissolve gallstones within the liver and be safe for patients.
•In rabbits, D-limonene (from citrus peels) synergistically combined with DMSO to dissolve implanted human gallstones.
•MTBE is sometimes infused into the gallbladder to dissolve cholesterol gallstones (comprising 80-90% of gallstones), but cannot dissolve the rarer pigment (bilirubin) gallstones. A series of Chinese studies demonstrated that once dissolved in DMSO, MTBE can (e.g., outside the body it dissolved 79.12% of the stones within 48 hours significantly outperforming other agents, and likewise in dogs, 76.83% of their stones were dissolved after 63 hours). Finally, a third formulation that also included cyclohexane diamine tetraacetic acid showed an even greater ability to dissolve these gallstones.1,2,3,4
Note: these studies repeatedly emphasized that these formulations were safe and showed no toxicity. I am skeptical of this, as MTBE alone is quite toxic (e.g., due to side effects, it was largely withdrawn from medical use a decade ago), and it is quite possible that combining it with DMSO would increase rather than neutralize its toxicity.
•In 50 patients post-emergency surgery for appendicitis or cholecystitis, 50% DMSO reduced postoperative wound complications to 4%, compared to 14% with 30% DMSO and 24% with traditional methods.
•One safety study injected DMSO directly into the biliary tree of mice (as sludging of bile in this region can lead to challenging gallstones). That study found that 50% DMSO caused no irritation, but 65% did (e.g., liver enzymes were elevated and necrosis, inflammation and fibrosis were observed). However, the irritation caused by 65% was transient and the rest of the bowel was not affected. Given that direct injections of 50% DMSO caused no issues and typically much lower concentrations of DMSO will typically contact the bile tract, this suggests DMSO is safe to administer into the biliary tract (to treat challenging conditions there).
Pancreas
DMSO (7-16%) has been shown to rapidly permeate the pancreas and shows promise for diabetes and pancreatitis.
Diabetes
Some Type 1 and Type 2 diabetics have reported that DMSO reduces (but does not eliminate) their need for insulin and that DMSO is particularly helpful for the condition since it can also alleviate the pain from diabetic peripheral neuropathy. Studies in this area include:
•Alloxan is toxic to the insulin-producing cells of the pancreas and can be used to induce diabetes. A 1977 study found that when DMSO was injected before administering alloxan, the animals did not develop diabetes (although a higher dose of alloxan caused the DMSO dose to provide only partial protection against diabetes).
•Type 1 diabetes results from the immune system attacking the insulin-secreting cells of the pancreas. One strategy for treating type 1 diabetes is to transplant healthy insulin-secreting cells into the pancreas. Unfortunately, this strategy often fails because the immune system will attack the transplanted cells too. However, in a mouse study, DMSO was found to protect those transplanted cells by decreasing IFN-γ expression and the number of dendritic, CD8, and Th1 immune cells while increasing Treg cell differentiation—all of which suggest that DMSO prevents spontaneous diabetes and autoimmune recurrence of type 1 diabetes.
•In both rabbit and rat bone marrow stem cells, DMSO combined with high glucose, boosted key insulin-promoting genes (e.g., Pdx-1), within 3 days, transforming these cells into clusters of insulin-producing islet-like cells. Furthermore, in the rat cells, by day 10, insulin, glucagon, and somatostatin were produced (with insulin secretion increasing from 5.56 to 24.5 μU/mL under high glucose conditions).1,2,3
Note: while diabetes due to a loss of insulin producing cells is typically associated with type 1 diabetes, this loss also contributes to type 2 diabetes (particularly as it becomes more severe). As such, DMSO potentially facilitating the body to replace them is quite noteworthy.
•GLP-1 is a key hormone the body uses to regulate satiety and blood sugar (and which diabetes drugs like Ozempic mimic). One study found that 0.5-2.5% DMSO increased GLP-1’s production of insulin by 2-2.5 times. The study’s findings suggest DMSO could help treat diabetes or allow GLP-1 users to use a lower dose of the medication.
•Exposing insulin-secreting cells to DMSO was found to enhance glucose-induced and tolbutamide-stimulated insulin secretion without significant effects on basal secretion or potassium responsiveness. Conversely, another study found that at high doses, DMSO would inhibit insulin secretion (however that inhibitory dose is much higher than a DMSO user’s pancreas would ever be exposed to).
Note: in their clinical investigations, Merck reported DMSO potentiated insulin and according to a DMSO author (I consider reliable) on the package inserts of DMSO preparations such as “Infiltrina” which were sold in the 1970s and 80s, the following was stated in the side effects section “Effects: Increased effectiveness of insulin,” which is suspect is due to DMSO’s protein stabilizing qualities improving the functionality of the insulin receptors (but could also be due to a variety of other mechanisms).
Pancreatitis
Pancreatitis is often quite challenging and dangerous as there are no conventional treatments for it (outside of cases where an obstruction causes it)—rather hospitals can only support the patient until they recover. Fortunately, DMSO (and ultraviolet blood irradiation) have been shown to be quite effective for treating it. For example:
•After inducing pancreatitis in rats, DMSO was found to improve pancreatic microcirculation and reduce ICAM-1 expression (a key part of the disease process) and subsequent leukocyte adhesion.
•Another mouse study found DMSO significantly reduced the pancreatic edema resulting from dietary induced pancreatitis.
•In rats, DMSO treated acute hemorrhagic necrotizing pancreatitis (a condition which typically has a mortality rate between 25-40%).
•A rat study found DMSO protected the pancreas from cerulein induced pancreatitis.
•A randomized double-blind trial took 78 patients with chronic recurring pancreatitis (and no other confounding gastrointestinal disorders) who presented within 2 hours with signs of pancreatitis but did not have signs of generalized peritonitis. Of them, 26 received 10% DMSO rectally, and at least 57% were pain-free after 12 hours (compared to 17% of controls), and all were pain-free after 24 hours (whereas 48% of controls were still experiencing pain). As a result, all DMSO subjects were discharged within 3 days, whereas only 22% of the control subjects were discharged within 5 days of hospitalization.
•In patients with recurrent pancreatitis, DMSO combined with allopurinol enhanced the efficacy of narcotic analgesics, significantly reducing pain, white cell counts, and serum lactate dehydrogenase levels (indicative of reduced pancreatic and peripancreatic inflammation and necrosis) compared to controls.1,2
•In three patients with chronic alcohol-induced pancreatitis, rectal DMSO achieved complete pain relief within 12 hours and resolved epigastric tenderness by day four, compared to persistent pain with placebo (pethidine, hyoscine, metoclopramide). No comparison was reported between DMSO alone and DMSO with allopurinol.
•The tissue injuries from abdominal surgeries can sometimes trigger pancreatitis. DMSO with fluorouracil effectively prevented and treated acute postoperative pancreatitis (mirroring another study which found DMNO reduced the oxidative stress that followed part of the liver being surgically removed).
•A Brazilian study found that DMSO reduced the oxidative stress that followed part of the liver being surgically removed.
Note: one author advocates combining IV DMSO with chlorine dioxide (given at a much slower drop rate) for pancreatitis—a combination, which as I show here, has had success in a wide variety of medical conditions.
Hemorrhoids
In many cases, congested blood will cause compromised veins to swell, which once severe, create significant issues for the patient. Unfortunately, as existing medical therapies have insisted on using external pressure and surgical intervention to address these disorders for decades, the results of conventional care for conditions like varicose veins have remained lackluster.
As DMSO can address many of the root causes of these venous disorders, it has long been observed to produce dramatic results for venous disorders, particularly varicose veins (detailed here) and hemorrhoids—and I’ve now had dozens of readers report massive improvements for each.
Note: while DMSO alone (or one of the other natural agents which effectively address the congestion within the blood) often can treat either condition, in particular varicose vein and spider vein cases, a natural therapy needs to be combined with DMSO to treat them, and likewise, nutritional supplementation to restore the blood vessels (detailed here) is sometimes required.
My husband (very skeptical) used it topically on his hemorrhoids and reported a significant reduction in size after the first application. He just needs to keep using it consistently.
Two friends of mine had their hemorrhoids vanish after a single subcutaneous thigh injection of DMSO. They both had had them for many years, one of them for 15 years, and now they're completely clear.
In turn, many readers, like the above ones, have reported significant success treating hemorrhoids with topical DMSO, injected DMSO or DMSO suppositories (e.g., consider these ten stories1,2,3,4,5,6,7,8,9,10,11) with the pain often completely disappearing and the hemorrhoids shrinking or vanishing.
Note: while Stanley Jacob (the pioneer of DMSO) treated hemorrhoids with DMSO, another author used DMSO to treat them, and Merck reported that it improved recovery after their surgical removal. I am not aware of any published studies that directly assessed DMSO’s use for hemorrhoids.
Lastly, there is also significant data (summarized here) that DMSO, through the same mechanisms it heals organs within the gastrointestinal tract, also greatly benefits a variety of prostate conditions, including prostatitis and benign prostatic hyperplasia (BPH). As such, the DMSO community routinely uses DMSO to treat prostate issues (frequently with combination DMSO suppositories or enemas, as that gets DMSO the closest to the prostate) and many readers have also reported dramatic improvement in prostate issues, particularly enlarged prostates.1,2,3,4,5,6,7,8
Treating Gastrointestinal Disorders
If you take a step back, the results consistently demonstrated with DMSO for GI issues are remarkable and merit being immediately adopted into the standard of care, particularly since it can safely treat many conditions medicine struggles with and frequently are fatal for patients. Nonetheless, as we’ve seen time and time again, this never happens (e.g., DMSO being adopted by our hospitals would greatly reduce the heart-wrenching and costly disability and deaths which follow strokes, spinal cord injuries, and head trauma—yet despite decades of data supporting it, no American hospital does this).
For this reason, it's essential that each of us know how to administer it ourselves, so we aren't left at the mercy of a medical system that prioritizes existing protocols over exploring unorthodox approaches that may benefit patients who don't respond to conventional treatments.
In the final part of this article, I will review:
•The existing protocols for using DMSO to treat the gastrointestinal conditions discussed throughout this article (including hemorrhoids, prostatitis, and BPH)
•Other natural therapies we find are frequently necessary to resolve chronic gastrointestinal issues (e.g., cholecystitis, Crohn’s or ulcerative colitis, leaky gut, and acid reflux)
•Guidance for DMSO enemas and suppositories
•More general information on how to use DMSO for individuals wishing to use it for other issues (e.g., pain) and where to obtain it (remarkably despite DMSO costing almost nothing, a striking number of counterfeit and scam DMSO products are starting to emerge—which is sadly a testament to the world we live in).
Source: https://www.midwesterndoctor.com/p/how-dmso-heals-the-gut-and-cures
Original Article: https://www.lewrockwell.com/2025/09/no_author/how-dmso-heals-the-gut-and-cures-gastrointestinal-diseases/
Note: We have not reviewed all of the links in this article. Usually we remove the links if we have not reviewed them. In this article we are keeping them here as they lead to many studies, although we have not verified each link or study.
Related:

Comments ()